

Comatose in Memory Care
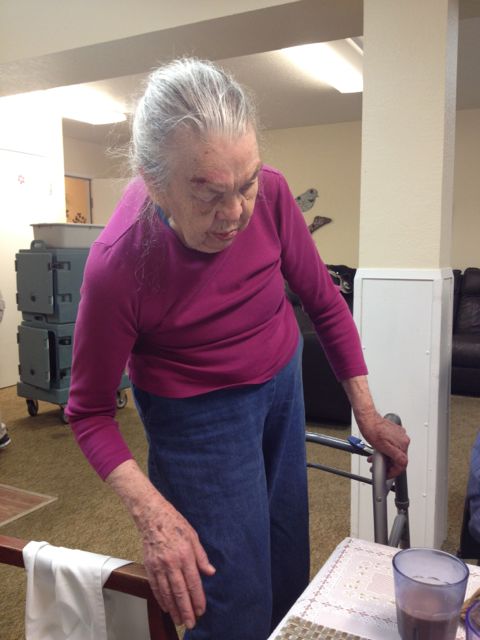
My mother-in-law who got over drugged in the hospital several months ago is now in her second memory care community in Seattle. The first high-end memory care community in downtown Seattle wanted to follow the doctor’s recommendations of sedation. It took me three days to get the drugs reduced by half after I saw my overmedicated mother-in-law. Then the second memory care community promised our family that they would get her off the reduced Haldol dose. We believed them and paid a hefty community fee (a one time move-in fee) Sigh…
It’s been almost two months in the second Memory care.
We had an unproductive care conference about two weeks ago. When the family talked about changing the psych drugs the conversation led to considering Amy as a candidate for hospice because she was not eating. What? It turns out one of the drugs she began in the hospital was also an appetite suppressant.
She was overmedicated in the hospital because there were no rooms in the psych ward, so my mother-in-law stayed in the emergency room for three days and two nights. Getting the picture of sedation now?
My sister-in-law is on the warpath. She is demanding changes for her mom and talking about moving her to a third place. Will it help?
The second memory care called my husband to see if they could save the move out. He simple said, “You have known that the family wanted my mom off the Haldol. How many phone calls and faxes have you made to the doctor to make that happen?” The administrator started to back pedal.
My sister-in-law took my mother-in-law to her doctor yesterday. A 15-minute appointment turned into nearly hours. The doctor is going to take her off the Haldol but does not have a clue what medications will help or are necessary. My mother-in-law has significant dementia, and seemed to have had a psychotic break when she lost her home of 50 years and her husband within a week.
Why is it so hard to unsedate a senior who cannot speak on his or her own behalf? Is it easier for the memory care staff if the residents are half sedated? Can anyone help us on how to turn this around? Any tips on psychotropic drugs? Which ones are best?
Don’t wait until you’re in a health care crisis like author Diane Masson’s in-laws. It has been a nightmare for her in-laws and all the adult children. Learn how to plan ahead like Masson’s mom. Research your future choices NOW to avoid being “put” somewhere, or having decisions made for you by others. “Your Senior Housing Options” is a new resource book available on Amazon.com with a 5-star rating. It offers a step-by-step guide to the options, including staying home.
Seniors, Boomer children, spouses, family members and caregivers are desperate to learn how to truly differentiate good senior housing from mediocre at best. Diane Masson’s new book will answer these heart-wrenching issues in an easy, simple, story telling format with humorous illustrations.
Diane has worked in senior housing for 17 years and is the regional marketing director for two debt-free Continuing Care Retirement Communities in Southern CA (Freedom Village in Lake Forest and The Village in Hemet). Her first book “Senior Housing Marketing – How to Increase Your Occupancy and Stay Full,” is being utilized by senior housing professionals across the country.
For weekly tips and advice go to www.Tips2Seniors.com and learn more from author and senior housing expert Diane Twohy Masson.

Why don’t you stay Home Instead?
Logical question. So many reasons including eloping. Please read previous blogs for the full picture.
First of all I want to say my heart reaches out to you and your family. My experience with residents like your mother include two options: 1. Admit mom to a geriatric psych hospital. This is not an easy step and certainly not a guarantee of success. Communication with the hospital team can be difficult but so is the condition surrounding mom. 2. Place mom in a memory care facility where an experienced long-term care medical team rounds weekly and the memory care staff is experienced with managing residents like your mom. Many times the best medicine is a consistency of surroundings and time. I wish you the best.
Thank you Jim. First, we did admit her to a geriatric psych ward of a hospital. This is where the drugging began. Second, after the respite stay, we placed her in a secured memory that with an experienced nurse and administrator. They assured us that they would get her off the Haldol. No real effort was ever made. The family made a mistake in believing in their experience and waited for them to work with the doctor. At a care conference we were led to believe that a change in drugs would happen too. A week later, no change, so my sister-in-law scheduled to take my mother-in-law to the doctor. The doctor does not understand all the medications. So he ordered no more Haldol in three days so a psych nurse could go evaluate my mother-in-law when she was still on Haldol. The nurse is selecting the drugs? The conversation that the family had with the doctor of having her on nothing seems to have evaporated. How do you work the doctor/HMO system?
Diane, how unfortunate and how common, that I have heard these same comments. It seems you have taken some really great steps, but not working out for her. When she was taken to the “doctor”, was it her family MD or was it a Geriatrician? A Geriatrician is much more knowledgeable about the effects on medications regarding interactions, length of time to have those meds reduced, combined with the disease process. Ensure that the MD is a board certified Geriatrician and insist on the MD seeing her in lieu of the NP or PA. As you know, not all dementias are necessarily psych issues. It is common for the first thing we do is put them on Haldol, which is contraindicated in the elderly. According to the FDA: WARNINGS – Increased Mortality in Elderly Patients with Dementia-Related Psychosis – Elderly patients with dementia-related
psychosis treated with antipsychotic drugs are at an increased risk of death. HALDOL Injection is not approved for the treatment of patients with dementia-related psychosis.
I don’t know her exact diagnosis, but there are alternatives to Haldol, for sure. Activities centered around her diagnosis, redirection, and on and on.
Please let me know if I can provide any assistance or guidance. As you know, you have to take control of the desired results. Don’t take no for an answer.
Carole Campbell, RN, NHA, CCM has been in the Long Term Care arena for 25+ years and has operated multi-skilled nursing facilities for some of the largest post-acute providers in the nation. She has served as a staff nurse, DON, NHA, Certified Geriatric Care Manager and Regional Director of Operations.
Let me clarify that Haldol is not contraindicated in all elderly as I noticed that I should have stated that more clearly. I would surely be really careful before it was used though and under strict supervision and oversight.
Thanks Diane – my thoughts are with you.
Hi Diane,
What a very difficult situation. As a registered nurse and a private case manager, my suggestion would be to have mom-in-law evaluated on an outpatient basis by a geriatric psychiatrist. These physicians are most capable of evaluating medications, making recommendations based on expertise in seniors and behavioral medications, and can advocate with your family to the facility and the primary care physician about an appropriate plan of care. Typically these specialists are difficult to get an appointment with, so it would involve keeping mom-in-law at her second facility until she could see the physician.
Another option would be to have her committed in an inpatient psych hospital – I would recommend asking local experts to find one which specializes in the geriatric population. They can try to straighten out her medications in the meantime and she could still see the geriatric psychiatrist in the meantime.
Another suggestion is to speak with the pharmacist or primary care physician about the current medication regimen and side effects. There may be other medications besides the Haldol that are causing sedation and I would ask for the entire list to be reviewed.
Also, I think it is good for you to know that the state has tight regulations regarding keeping psychiatric and sedating medications to a minimum. I am not sure why both facilities believe so strongly in medicating mother-in-law but it may be that they are not suited in our non-pharmacologic ways to deal with dementia patients. How much experience and expertise do these facilities have with same? You may want to point out to the facilities the state regulations stating residents have a right to receive as little medication as possible.
Good luck, I will hope for the best for you, your family, and mother-in-law.
What was the reason your Mother -in -Law was originally hospitalized? Who diagnosed her as a psychiatric patient? Did she present with aggressive behavior? I really think that she was given Haldol probably to quiet her down, but if she was parked in a busy corridor, with lots of traffic, given that she was probably scared and confused, her symptoms might have been purely a result of dementia and not a psychiatric episode. In which case Haldol should not have been used. She probably needed to be treated with more focus on what produced her symptoms!