by Diane Masson | Jul 5, 2015
Professionals have told me that a trauma could have caused Amy’s dementia (my favorite mother-in-law) to escalate rapidly. Is this true? Can all the dementia professionals and family members weigh in with their experiences?
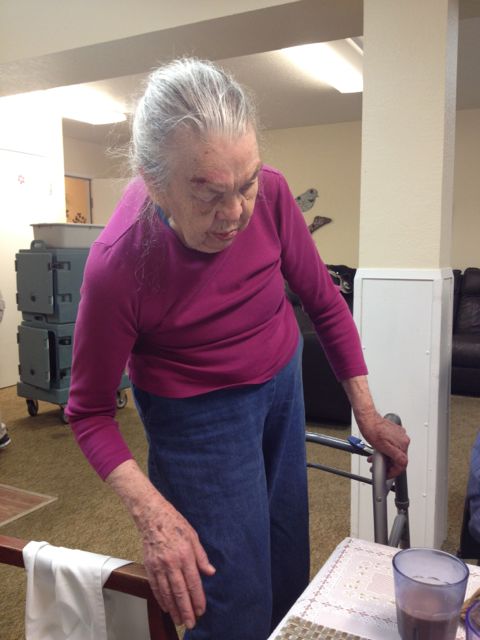
My mother-in-law’s dementia was progressing slowly like my mom’s vascular dementia. There are four stages of memory loss and Amy was in stage 2, before the trauma. She repeated herself a lot, needed cueing for personal hygiene, medication management and had little desire to leave the home. Amy talked about not being able to remember stuff, but she could still read the paper, dress, bathe, toilet and feed herself.
Then Bill, my favorite father-in-law and Amy’s 24-7 caretaker, had a heart attack and went to the hospital. Amy could not understand where her rock and husband of 65 years had gone. She ended up having a psychotic break and eloping (The police had to find her and bring her back home.). A whole series of dramas happened and she hit a nurse. Then she too was hospitalized and put on psychotropic medications. Amy was in the hospital for three weeks in the psych ward.
By the time she got out of the hospital, the Amy I had seen months earlier was gone. The first time my husband and I saw her after the hospitalization (we live three states away) was so sad. The vivacious and sarcastic Amy was gone. It was like seeing a shell of her former self. Her lip trembled, her arm shook and she was so sleepy from the Haldol drugs. We immediately got the psychotropic medication reduced by half. It took us another three months to get her completely off the Haldol because we are not Amy’s Power of Attorney.
Amy was suddenly in stage 4 dementia. She needs help with absolutely everything and is not able to communicate her thoughts or needs. Hospice has been discussed in care plan meetings.
Has anyone else seen such a rapid decline with a family member or resident with dementia? Was it losing her husband, the psychotropic medications or both that caused Amy’s rapid deterioration? I believe that if my in-laws had planned ahead and moved into a Continuing Care Retirement Community (CCRC) that staff and residents would have supported Amy when her husband was first hospitalized. The CCRC would have rallied around her, helped her transition to the care level she needed and her world wouldn’t have changed so dramatically (she would have been dining daily with resident friends instead of being isolated in her own home).
What do you think?
“Your Senior Housing Options,” has a simplistic title, but what’s inside this new book can save a you months of research time. Hear Diane Masson’s interview of how her mother and in-law’s faced the pivotal decision to plan ahead or wait until a crisis. Learn the pitfalls from transitioning from your home to senior housing. Understand what questions to ask, insider tips and dirty secrets revealed. The decision to stay home requires caregivers. Prevent elder abuse by determining if a home care agency is reputable, before they move into your home. You are just not looking for today’s needs, but for your future care. Discover key differences between rental facilities vs Continuing Care Retirement Communities. Do you have enough financial resources if you need to be in a higher level of care for an extended period of time? For weekly tips join at: Www.Tips2Seniors.com
Diane Masson has worked in senior housing for 17 years and is the regional marketing director for two debt-free Continuing Care Retirement Communities in Southern CA (Freedom Village in Lake Forest and The Village in Hemet). Her first book “Senior Housing Marketing – How to Increase Your Occupancy and Stay Full,” is being utilized by senior housing professionals across the country. Both her first book and second book, “Your Senior Housing Options,” have a 5-star rating on Amazon.com.

by Diane Masson | May 31, 2015
Will the POA understand new shoes are needed?
It’s hard to be an advocate for a senior for years on end. I advocated for my own mom (with vascular dementia) for over 10 years, until I recently lost her. Advocacy is not an easy job and it can entail sleepless nights of concern.
It’s vital to select a Power of Attorney (POA) who currently knows you well enough. If you can no longer speak on your own behalf, your POA needs to know if you are over medicated or sedated just by looking at you. They need to know your baseline so they can help you and reverse the issue or accelerate an outcome in a timely fashion.
The POA’s main purpose is to comply with your wishes that were indicated before you became incapacitated. They should always protect your best interests both mentally and physically.
Over medication is a growing problem for seniors. I have heard many stories of hospitals overmedicating seniors. My own mother-in-law was over sedated in the emergency room. She has Alzheimer’s. They had no room in the psych ward and she was drug restrained for three days and two nights in the emergency room. Sigh…
It has taken us four months to get my mother-in-law off Haldol. Psychotropic drugs and dementia do not mix well. Her POA thought the doctors understood what they were doing tapering off the medication. Unfortunately, my mother-in-law’s doctor admitted to knowing nothing about psychotropic drugs and was relying on others to advise her. Gulp… What a mess! We are talking about seniors’ lives…
Neither the doctor nor the POA knew what to do about my mother-in-law’s medications or where to begin. It literally required a family member taking my mother-in-law to her doctor and demanding, in person, for the Haldol to terminate immediately. The doctor could see for herself the sedation instead of relying on the input from home health professionals. The weird part was the doctor agreed to terminate the Haldol in three days. We wondered why wait three days? It turned out she wanted a psych nurse to visit my mother-in-law while she was still on the Haldol. The psych nurse agreed to terminate the Haldol too. Here is the horrible part; the psych nurse ordered a different psychotropic drug on an as needed basis. What?? It took the family helping the POA another week to reverse that fiasco.
Why are doctors prescribing psychotropic drugs to seniors with dementia in the first place?
A POA needs to be vigilant. It may require educating themselves about medications that they no nothing about. Very few POA’s are doctors and nurses. If you are the parent of a doctor or nurse who will be your POA, then congratulations are in order for you.
What about a senior with neuropathy in his or her feet? Something as simple as buying quality shoes, so a senior has better balance is key. Will the POA do it?
What if your POA is an attorney or an absentee POA relative who rarely visits, how can they understand or advocate for your needs?
A POA needs to be willing to speak to the doctor on your behalf. Some possible POA’s are very direct (speak their mind) and others are indirect (prefer to fade into the background). Some folks are introverted and others are extroverted. Who are you asking to be your POA? Will they get the job done? This is not a position for sissies. Your POA needs to be hardcore if you are in dire need. Your POA may have to spend relentless hours pursuing a medication result that is beneficial for your needs.
What have you encountered? Who have you selected to be your POA? Do you feel good about your decision?
Don’t wait until you’re in a health care crisis like author Diane Masson’s in-laws. It has been a nightmare for her in-laws and all the adult children. Research your future choices NOW to avoid being “put” somewhere, or having decisions made for you by others. “Your Senior Housing Options” is a new resource book available on Amazon.com with a 5-star rating. It offers a step-by-step guide to the options, including staying home.
Seniors, Boomer children, spouses, family members and caregivers are desperate to learn how to truly differentiate good senior housing from mediocre at best. Diane Masson’s new book will answer these heart-wrenching issues in an easy, simple, story telling format with humorous illustrations.
Diane has worked in senior housing for 17 years and is the regional marketing director for two debt-free Continuing Care Retirement Communities in Southern CA (Freedom Village in Lake Forest and The Village in Hemet). Her first book “Senior Housing Marketing – How to Increase Your Occupancy and Stay Full,” is being utilized by senior housing professionals across the country.
For weekly tips and advice go to www.Tips2Seniors.com and learn more from author and senior housing expert Diane Twohy Masson.

by Diane Masson | May 17, 2015
Drug Restraints and the Haldol Shuffle
Adult children just want their parent with dementia to be okay. Most do not have a clue on psychotropic (mind altering) medications or how they work. Families rely on professionals to recommend doses and medications for their senior parents. If a professional doctor or memory care community says that our mom or dad needs these medications, we tend to accept their wisdom. We are programed to not question authority. Yet when a parent is sedated in a drugged stupor over an extended period of time, more adult children are starting to ask why. At this point it can be too late for a senior with dementia.
Psychotropic medications can have a lasting affect on a senior with dementia.
Seniors may never be able to return to their baseline, before taking psychotropic drugs. My mother-in-law was given Haldol and now does the Haldol shuffle. It is a continuous stand up, walk, sit down and then it starts all over again. It is so sad to watch and they can’t stop. A professional told me it’s like their skin is crawling and they have to keep moving to make the feeling go away.
When we recently brought my mother-in-law her favorite Greek food for lunch, she sat down in front of her favorite foods at the table and then immediately stood back up and started the Haldol shuffle again. She had no desire to eat her favorite foods.
It has taken four months for the family to get her off the Haldol. My sister-in-law had to physically take my mother-in-law to her primary care physician and demand for the Haldol to be discontinued last week. The doctor was shocked my mother-in-law had been on Haldol for such a long period of time, with no recorded outbursts requiring such a strong medication.
So what happened?
My father-in-law, Bill, and mother-in-law, Amy, refused to move from their home of 56 years. Bill had been Amy’s caregiver for the last four years because she had dementia. When Bill had a sudden heart attack and went to the hospital, Amy was in jeopardy in the family home. The local children rallied around the dad in the hospital. For all intensive purposes, Amy was left alone for three days and three nights. My husband and I live 1000 miles away and we hired a geriatric care nurse. Amy was having delusions, not recognizing her own children, making unsafe choices, refusing to take her medications and eloped (she walked away and the police brought her home).
No community would accept her without medications
No assisted living would take her, because she had eloped. A memory care community came to assess whether they would accept Amy and said they would not take her unless she was medicated. The family understood drugs were a requirement at this point. My sister-in-law called Amy’s doctor’s office and explained Amy symptoms of delusions and etc., they did not want her in the clinic. Are you kidding me?!!? Amy’s doctor’s nurse said to take her to urgent care. But according to urgent care she was not bad enough to be admitted to the hospital. They sent her home with five pills of Adavan. Now what? Medications were required live in the memory care community. What could we do? She was not safe at home by herself and she didn’t want her adult children (she no longer recognized) to be with her. Finally a geriatric nurse provoked Amy to hit her. Then the police came and Amy was taken to the hospital by ambulance. There was no room in the psych ward so she was drug restrained in the emergency room for three days and two nights.
So the psychotropic nightmare began
The hospital said strong medication was necessary and started the Haldol. She was in the hospital for three weeks. Both memory care communities said the medications were necessary for Amy too. The family stupidly believed the professionals. Amy’s HMO had poor communication between the doctor, the hospital, the memory care communities and the home health professionals that saw Amy in person.
The first memory care community recommended making no drug changes for one or two months. When my husband and I flew to Seattle and saw Amy’s level of sedation, I said, “No way,” and fought to have the Haldol reduced by half. After the family figured out that the memory care community had no intention of supporting the reduction of medications, we moved Amy.
The second memory care community promised to reduce the psychotropic drugs and get her off the Haldol. Within two weeks they reduced the Haldol by half. Yet Amy was still in a drugged stupor. She was on a mix of AM and PM psychotropic drugs. This secure memory care community had a staffing ratio of one staff to ten residents.
We have since learned that drug restraints in memory care are common, particularly if they are short staffed.
I wrote this article to warn others adult children to demand reductions in psychotropic medications immediately. I am so sick of professionals saying to wait a month or more to see what happens with the medications. Then it’s too late. Amy went from fully toileting herself to incontinent. She went from eloping (walking away and the police brought her back) to barely walking. She went from smiling and talking to having a blank look on her face and staring into space.
We want to find Amy’s baseline again. She will never be at the same level of cognition from four months ago. There are moments and sentences were her personality returns. It is so sad to see her in this reduced state.
I am not saying that I am anti-drugs, but a Power of Attorney (POA) needs to be informed of the consequences of psychotropic medications. My own mother with dementia benefited from psychotropic drugs when she became very anxious and delusional in the later stages of her dementia. The price she paid for taking those psychotropic medications was permanently losing the ability to walk. I wish I had known then what I know now. Now my mother-in-law can barely walk…
Any hope? Have you had a similar experience with your parent? What happened? Have you witnessed drug restraints in memory care communities or hospitals? How can we stop it? How can a family find a good memory care that does not require drug restraints? What are the proper questions to ask?
Don’t wait until you’re in a health care crisis like author Diane Masson’s in-laws. It has been a nightmare for her in-laws and all the adult children. Research your future choices NOW to avoid being “put” somewhere, or having decisions made for you by others. “Your Senior Housing Options” is a new resource book available on Amazon.com with a 5-star rating. It offers a step-by-step guide to the options, including staying home.
Seniors, Boomer children, spouses, family members and caregivers are desperate to learn how to truly differentiate good senior housing from mediocre at best. Diane Masson’s new book will answer these heart-wrenching issues in an easy, simple, story telling format with humorous illustrations.
Diane has worked in senior housing for 17 years and is the regional marketing director for two debt-free Continuing Care Retirement Communities in Southern CA (Freedom Village in Lake Forest and The Village in Hemet). Her first book “Senior Housing Marketing – How to Increase Your Occupancy and Stay Full,” is being utilized by senior housing professionals across the country.
For weekly tips and advice go to www.Tips2Seniors.com and learn more from author and senior housing expert Diane Twohy Masson.

by Diane Masson | May 10, 2015
Comatose in Memory Care
My mother-in-law who got over drugged in the hospital several months ago is now in her second memory care community in Seattle. The first high-end memory care community in downtown Seattle wanted to follow the doctor’s recommendations of sedation. It took me three days to get the drugs reduced by half after I saw my overmedicated mother-in-law. Then the second memory care community promised our family that they would get her off the reduced Haldol dose. We believed them and paid a hefty community fee (a one time move-in fee) Sigh…
It’s been almost two months in the second Memory care.
We had an unproductive care conference about two weeks ago. When the family talked about changing the psych drugs the conversation led to considering Amy as a candidate for hospice because she was not eating. What? It turns out one of the drugs she began in the hospital was also an appetite suppressant.
She was overmedicated in the hospital because there were no rooms in the psych ward, so my mother-in-law stayed in the emergency room for three days and two nights. Getting the picture of sedation now?
My sister-in-law is on the warpath. She is demanding changes for her mom and talking about moving her to a third place. Will it help?
The second memory care called my husband to see if they could save the move out. He simple said, “You have known that the family wanted my mom off the Haldol. How many phone calls and faxes have you made to the doctor to make that happen?” The administrator started to back pedal.
My sister-in-law took my mother-in-law to her doctor yesterday. A 15-minute appointment turned into nearly hours. The doctor is going to take her off the Haldol but does not have a clue what medications will help or are necessary. My mother-in-law has significant dementia, and seemed to have had a psychotic break when she lost her home of 50 years and her husband within a week.
Why is it so hard to unsedate a senior who cannot speak on his or her own behalf? Is it easier for the memory care staff if the residents are half sedated? Can anyone help us on how to turn this around? Any tips on psychotropic drugs? Which ones are best?
Don’t wait until you’re in a health care crisis like author Diane Masson’s in-laws. It has been a nightmare for her in-laws and all the adult children. Learn how to plan ahead like Masson’s mom. Research your future choices NOW to avoid being “put” somewhere, or having decisions made for you by others. “Your Senior Housing Options” is a new resource book available on Amazon.com with a 5-star rating. It offers a step-by-step guide to the options, including staying home.
Seniors, Boomer children, spouses, family members and caregivers are desperate to learn how to truly differentiate good senior housing from mediocre at best. Diane Masson’s new book will answer these heart-wrenching issues in an easy, simple, story telling format with humorous illustrations.
Diane has worked in senior housing for 17 years and is the regional marketing director for two debt-free Continuing Care Retirement Communities in Southern CA (Freedom Village in Lake Forest and The Village in Hemet). Her first book “Senior Housing Marketing – How to Increase Your Occupancy and Stay Full,” is being utilized by senior housing professionals across the country.
For weekly tips and advice go to www.Tips2Seniors.com and learn more from author and senior housing expert Diane Twohy Masson.

by Diane Masson | May 3, 2015
Mean Mom, Nice Mom and Dementia
Here is a painful subject that I am going to bring up. Hundreds of people have reached out to me in the last week since my mother passed. So many of them shared a story about their own mom passing. Some were wonderful experiences that they will treasure and others were not. Sudden deaths are very hard. Every personal death I have experienced in my life was sudden, except for my mom’s death. You can read about my mom’s passing experience HERE.
You either had a loving caring parent or you did not. This article is for those who did not.
Many vulnerable sons and daughters were abused by either their mom or dad, sometimes both. We live in world that accepts dysfunctional families now. Family abuse that was hidden in the 1950’s and 1960’s can now be accepted in the mainstream. There are resources and counseling available so abused children (who have become adults) can acknowledge the abuse and move on.
My mother was abusive to all her young children. You can read my article MEAN MOM, NICE MOM and DEMENTIA HERE.
A wonderful counselor changed my life for the better and his recommendation is explained in my article MEAN MOM, NICE MOM and DEMENTIA HERE. My mom and I enjoyed over 20 years of a good adult relationship. I forgave her. Many of you know I have advocated for my mom’s care needs for the past 10 years.
So what happens if an abused adult son or daughter still has unresolved issues at death with mom? Do they go to the funeral? Do they have a free pass not to attend?
What have you encountered?
It seems ironic now, that my new book is dedicated to my mom. Writing this blog has been therapy for me over the last three years. After sharing numerous stories about my mom, several senior living people said you should write a book to help other seniors and their families. So I did and “Your Senior Housing Options” was published recently.
I love you mother and hope your stories peppered through the book can help others learn their options and plan ahead. So many seniors fight to stay home and then a sudden crisis causes them to lose their ability to choose like my in-laws did. What person in their right mind wants to be put someplace? My in-laws have no choices now. Seniors and their families should study the options and costs now. The greatest gift my mom ever gave me was to plan ahead at age 75, so her transition to assisted living was a good one. She recently passed at age 92 in skilled nursing care.
Diane has worked in senior housing for 17 years and is the regional marketing director for two debt-free Continuing Care Retirement Communities in Southern CA (Freedom Village in Lake Forest and The Village in Hemet). Her first book “Senior Housing Marketing – How to Increase Your Occupancy and Stay Full,” is being utilized by senior housing professionals across the country.

by Diane Masson | Apr 26, 2015
My Mom and I
My mother’s blood sugar spiked to 400 on Monday and 520 on Tuesday. She was fighting a UTI and ecoli. At 92, her body tried to fight it off. The doctor said the antibiotics would either work in two days or she would go down hill fast. It was the later.
The care ambassadors and nurses at Freedom Village were amazing. I lost count after twenty-three staff came in to say good-bye and provide loving care. One care ambassador said, “I’ve known your mom for two years and she was my family.” Another said, “Everyday she would greet me in the hall and compliment what I was wearing that day.” My favorite was someone reminding me of her love of cats and how she usually had one with her or would respond to the mechanical one that meowed, purred and moved. Her face would light up with joy.
My mom lived in a higher level of care for nine years. Seven years in assisted living and almost two years in skilled nursing in Lake Forest, CA. Six years ago, a doctor made a comment that her life was not worth living because she had dementia and couldn’t remember anything. I replied, “How many of your patients said thank you and complimented you today?” The doctor sheepishly said, “Only your mom.” I said, “Then she still is fulfilling her purpose isn’t she?” The doctor backed off and gave the best care until my mom left that Seattle hospital.
Through nine years of advocacy for my mom, I have done the best I was able, making decisions with the knowledge that I have. I am not a nurse and based my advocacy on her wishes and trying to keep her comfortable.
Extraordinary Versus Comfort Care
Hospice began on Tuesday and they were a Godsend. My husband was in Seattle saying goodbye to his dad on hospice when everything happened. A nurse, a social worker and a chaplain came from hospice to support my mom and me. I learned the differences between extraordinary care and comfort care at the end. The IV’s, antibiotics and unnecessary medicine disappeared. The morphine and adavan began.
Final Burst of Energy
After the chaplain said some beautiful words, my mom had what they call a “burst of energy.” I was holding her hand when she opened her eyes half way and said, “I love you,” seven times and “thank you” twice. Then she closed her eyes and the energy was gone. I will treasure that memory.
After she choked while attempting to eat, I said no more food. A caregiver patiently helped her drink some juice even though it took 15 minutes. That was the last time I saw her drink because she could not swallow again.
The turns every two hours caused her to cry out. The repositioning was to prevent bedsores. I called hospice when the gentle turns seemed to hurt her more and they said to reduce the turns to every three hours and give the morphine 20 minutes before. The nurses and care ambassadors were outstanding. This little tip made the gentle turns easier for her.
The last day, she started to moan with every exhale. I called hospice again. The gurgling in the throat had started and it was time to start the medication that helped with that. The director of nursing arrived before hospice and we started the PRN of morphine and adavan that had been preapproved by her wonderful doctor. Hospice increased the frequency of the medications to once an hour and said she was not to be turned again. Alleluia.
The director of nursing was there every hour to administer the comfort medications. I cannot say enough about the staff of Freedom Village Health Care Center and how they supported and loved my mom and I, to the end.
My husband came back from Seattle and the room filled with music. When the chaplain arrived they sang together and it felt like a send off party. Her doctor entered about this time, gave me a hug and said, “She is going out in style. I am so happy that she is comfortable.” A priest came to give her last rites. I said and prayed everything I wanted to with my mom and have zero regrets.
After nine hours, my husband and I decided to take a dinner break. The director of nursing said she would not leave my mother until we returned. Another change happened right before we got back.
The chaplain and hospice were called. The moan on each exhale came back and I requested more morphine for her. Her doctor gave permission. Chris and I sang a couple of songs to her. The chaplain arrived. I requested scripture and the chaplain was reading from the Gospel of John when she passed. God’s presence was in the room. She was comfortable and at peace.
Today is Sunday and I would normally go and visit with my mom. I wrote this blog to help me with my own grief today.
It seems ironic now, that my new book is dedicated to my mom. Writing this blog has been therapy for me over the last three years. After sharing numerous stories about my mom, several senior living people said you should write a book to help other seniors and their families. So I did and “Your Senior Housing Options” was published recently.
I love you mother and hope your stories in the book can help others learn their options and plan ahead. So many seniors wait until a crisis and lose their ability to choose like my in-laws did. The greatest gift my mom ever gave me was to plan ahead and move into a Continuing Care Retirement Community. Over 16 years, my mom had good transitions through three levels of care.

 Professionals have told me that a trauma could have caused Amy’s dementia (my favorite mother-in-law) to escalate rapidly. Is this true? Can all the dementia professionals and family members weigh in with their experiences?
Professionals have told me that a trauma could have caused Amy’s dementia (my favorite mother-in-law) to escalate rapidly. Is this true? Can all the dementia professionals and family members weigh in with their experiences?